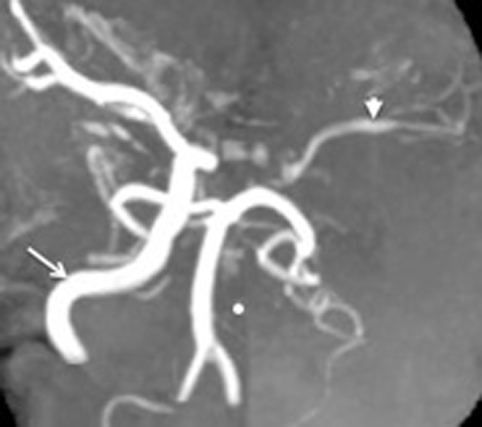
Figure 1. MRA demonstrating the absent Left ICA. The(•) highlights the site where the counterpart to the readily appreciated right ICA (arrow) should have been. The left MCA and its branches are visible (arrowhead), indicative of their reconstitution. The posterior circulation comprising of the two vertebral arteries confluencing into the basilar artery and their branches are also seen.
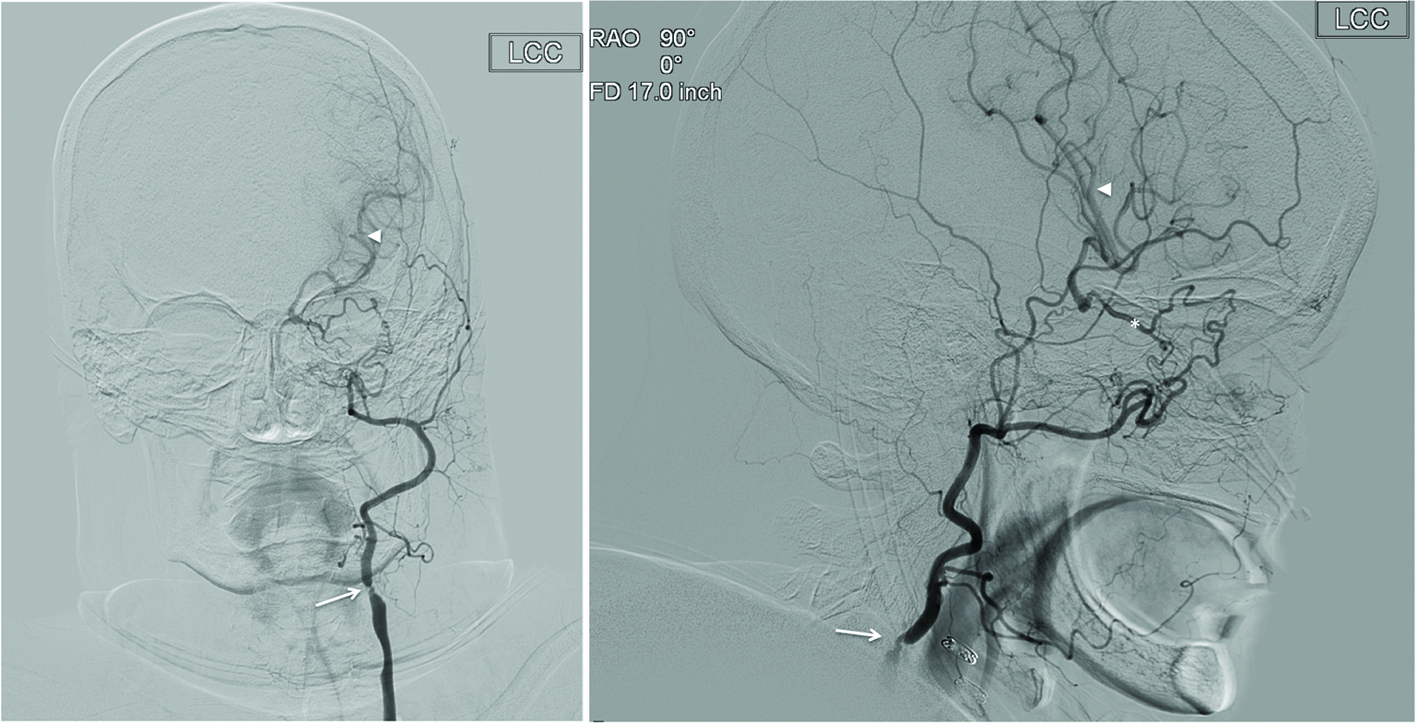
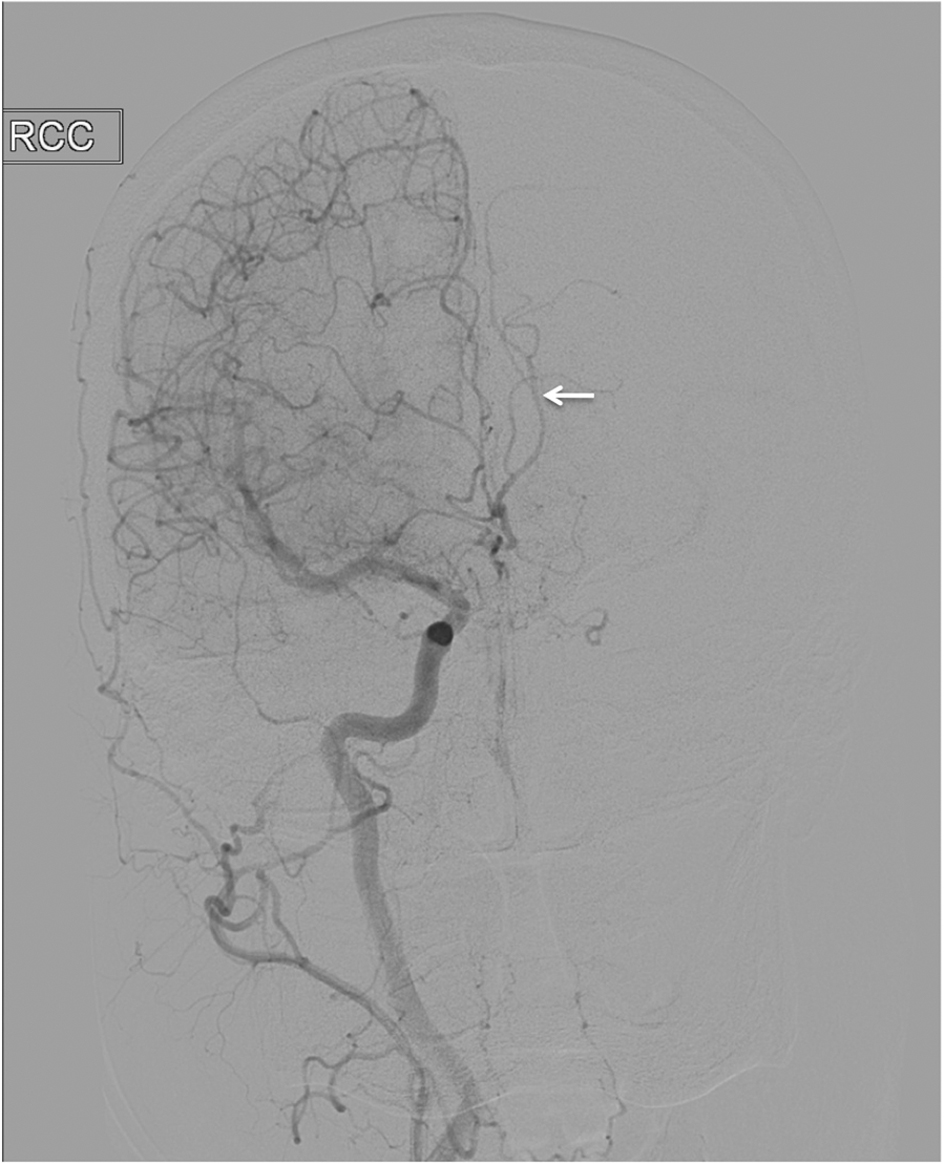
Figure 2. Catheter angiography of left common carotid artery in (a) anteroposterior and (b) lateral projections demonstrates the absence of left ICA. The ECA and its branches are appreciated. There is a severe stenosis of proximal ECA (arrow). The ethmoidal branches of the internal maxillary artery are anastomosing with the ethmoidal branches of the ophthalmic artery (*). The retrograde flow from the ECA via the opththalmic artery results in the reconstitution of the left MCA (arrowhead).