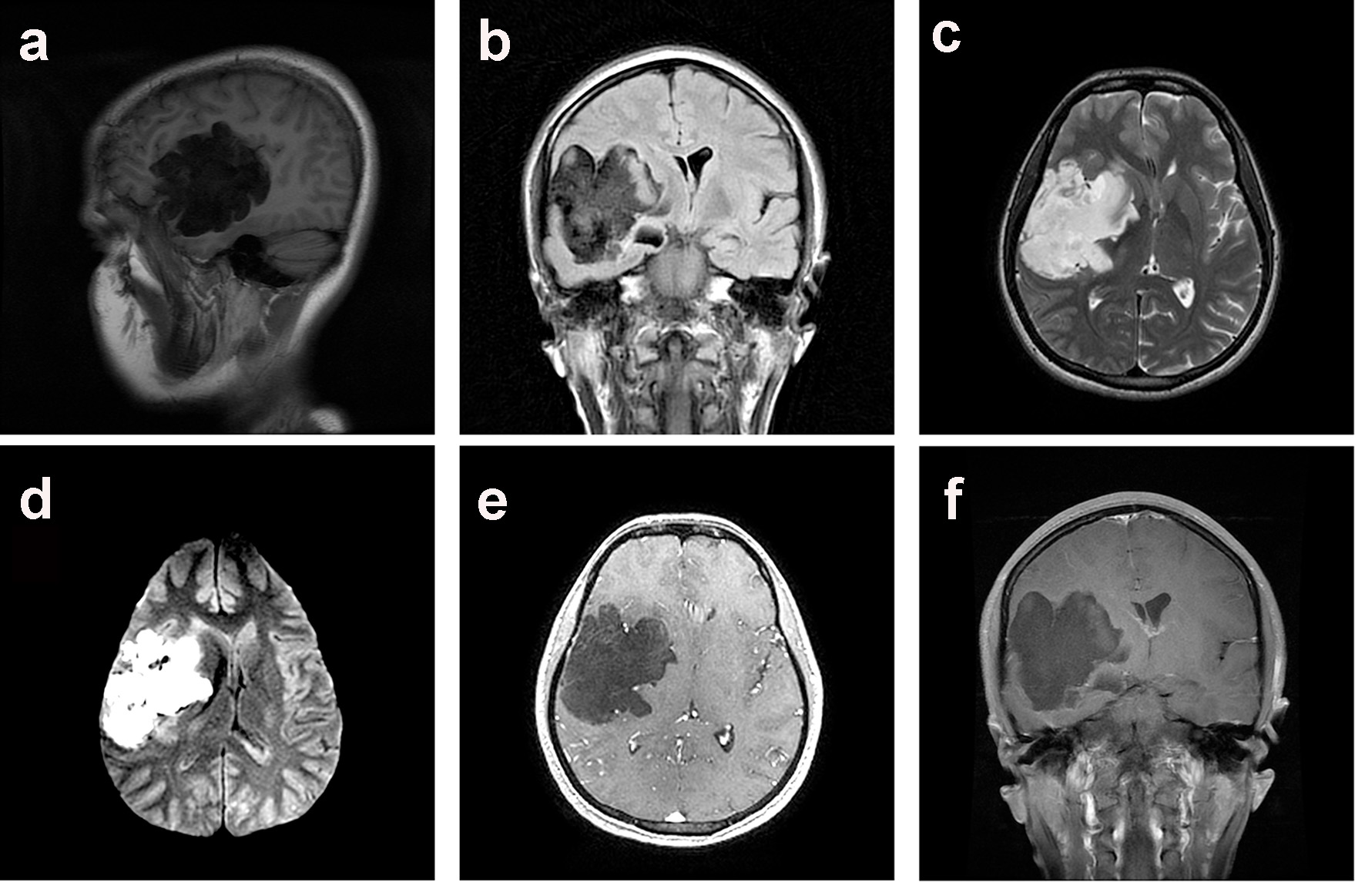
Figure 1. Preoperative MRI scan of the brain demonstrated a large right Sylvian epidermoid tumor. The lesion demonstrated a hypointense signal on para-sagittal T1-WI (a) and coronal (b) T2-FLAIR sequences, hyperintense signal on axial T2-WI (c) and axial DWI (d) MRI scan. There was no enhancement of the hypointense lesion following IV contrast as demonstrated on axial (e) and coronal (f) T1-WI MRI scan.
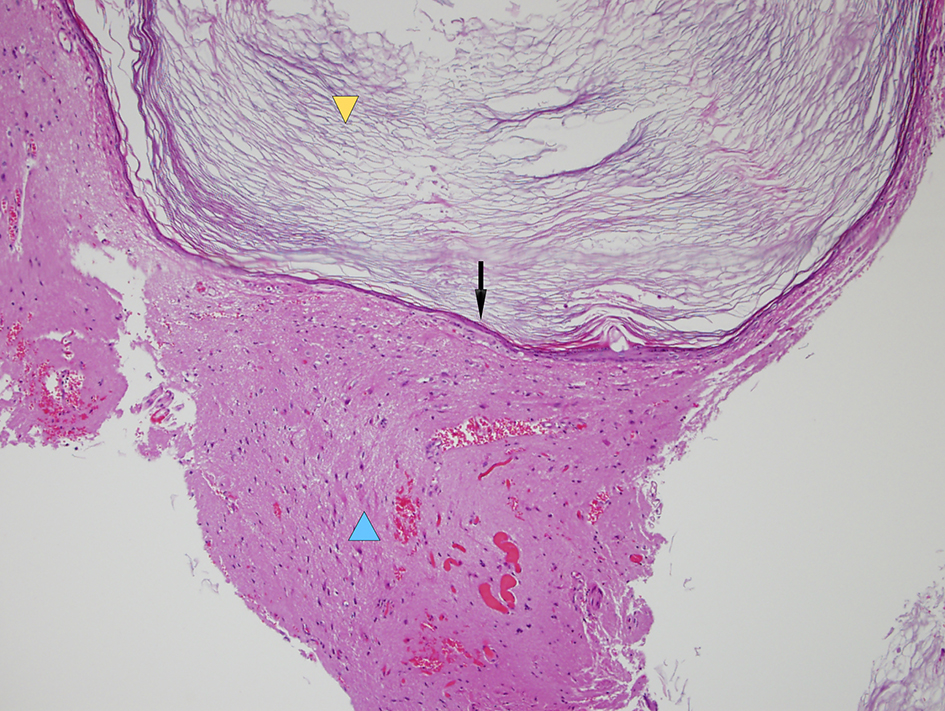
Figure 3. Histopathological microphotograph demonstrating a stratified epithelium wall (black arrow) containing keratin and cholesterol (yellow arrowhead) characteristics of an epidermoid cyst, and surrounding inflammatory cells and gliosis (blue arrowhead) (hematoxylin and eosin stain, × 100 magnification).
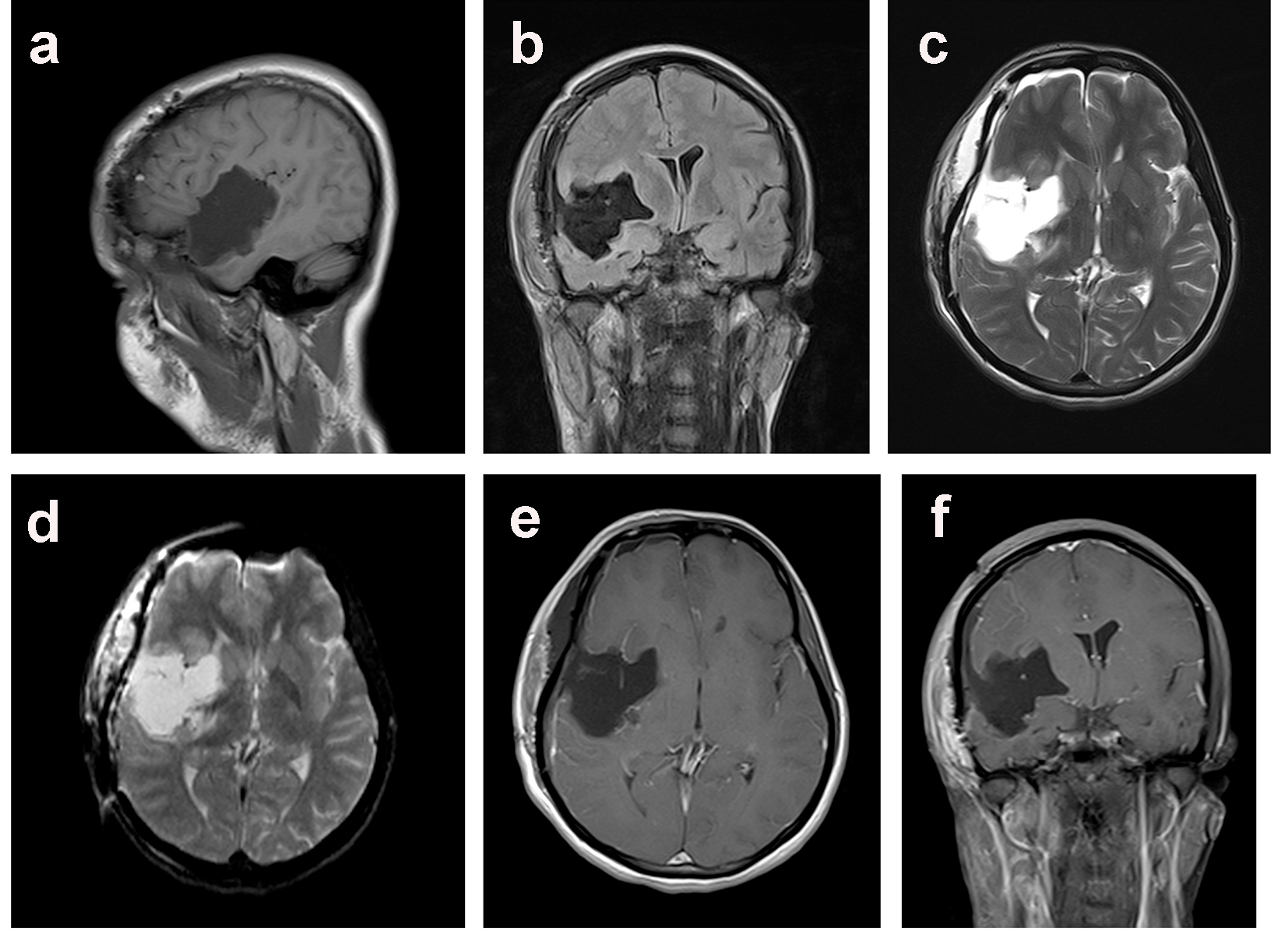
Figure 4. Postoperative MRI scan of the brain at 1 year follow up demonstrated complete resection of the epidermoid tumor as evidenced as a hypointense signal on para-sagittal T1-WI (a) and coronal (b) T2-FLAIR sequences, marked decrease hyperintense signal on axial T2-WI (c) and axial DWI (d) images. There were no vascular complications or enhancement of the hypointense lesion following IV contrast as demonstrated on axial (e) and coronal (f) T1-WI MRI scan.