
Figure 1. Robot-assisted therapy setup. The patient’s lower arm is supported in a trough and the hand placed around a joystick. The visual screen illustrates the reach-grasp-reach-release assisted therapy game, whereby repeated movements are made to 8 peripheral targets and back again to the central hold position. Both reaching of the shoulder/upper arm and the extension/flexion of the fingers and thumb are assisted and synchronised, such that the robot devices enable successful tasks to be completed even if the patient cannot move at all, for example at the beginning of the treatment programme.
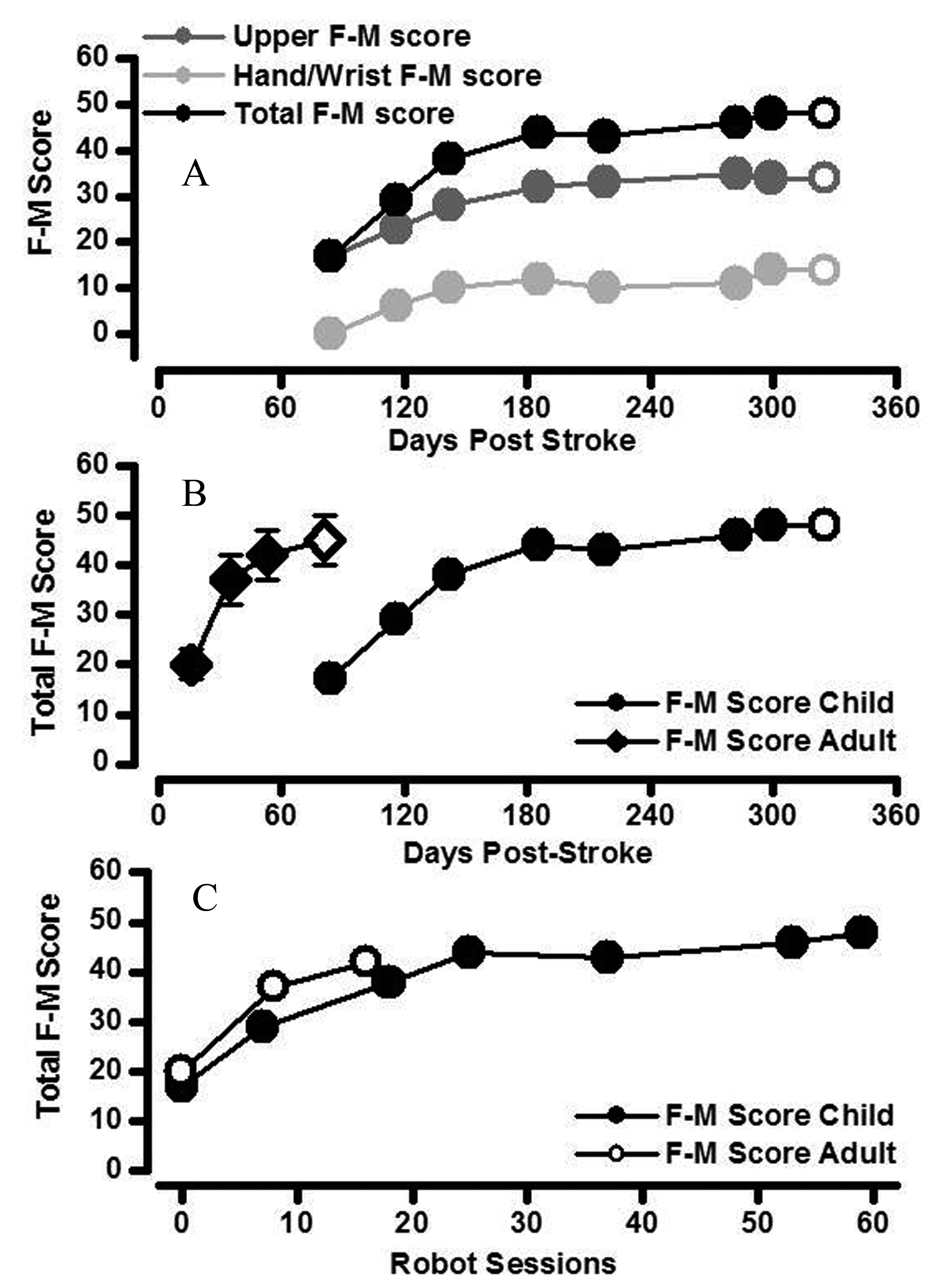
Figure 2. Changes in clinically assessed motor impairment. A. The increase in total arm F-M score (black circles) was the result of additive increases in both upper arm F-M score (score out of 42; dark grey) and hand/wrist F-M score (score out of 24; light grey) in the child stroke patient. Increases in arm segment F-M scores were maintained at one month follow-up in the child stroke patient (open symbols). B. Total F-M score for right upper limb of the childhood stroke patient (closed circles) increased relatively more quickly with time since stroke in the first half of the robot-assisted therapy (i.e. over first 3 months). The rate of increase in total F-M score with time since stroke for the child stroke patient was slower than that of a cohort of adult acute stroke patients (closed diamonds are mean ± standard error bars; N= 10) [9]. Increases in total F-M score were maintained at one month follow-up in both child and adult stroke patients (open symbols). C. The change in total F-M score was similar in child and adult stroke patients when compared as a function of robot-assisted therapy session number.